Informant: Self
CC: “My voice sounds different” x a few weeks (Hoarseness)
Diagnosis: Papillary Thyroid Cancer
HPI:
38 years old reliable female with no significant PMHx came to the clinic complaining of hoarseness for the past few weeks. The pt states that the hoarseness began 6 weeks and it is progressively becoming worse. Pt describes the voice as raspy and rough as it sounds strange to her ears. The pt states, she has tried to alleviate the voice changes by drinking tea and warm water with no relief. Along with the hoarseness, pt complains of pain with swallowing solid foods. The pain with swallowing began before the voice change but pt is more concerned regarding her voice change as the swelling pain only occurs with solid foods. The pain is non-radiating and nothing makes the pain better. Pt rates the pain 8/10 at its worse and 4/10 at its best. Pt admits to having mild SOB and fatigue after a long day of work. Pt denies any weight loss or gain, chest pain, excessive sweating, tremor, N/V/D, constipation, irritability, bone pain, anxiety, depression, or any other symptoms.
PMHx: none
Surgical Hx– appendectomy at age 26 with no complication
Family Hx: – Mother has Hypothyroidism and father has HTN
Social Hx – denies smoking, drinking or illicit drug use
Fiona is a 38 years old white female who works as a radiologist assistance in the QHC hospital
Allergies: PCN rash
Medications: Birth control pills and multi-vitamin pills
ROS:
HEENT: Denies ear pain, hearing changes, facial pain, c/o dysphagia for solids foods
Neck: denies stiffness or swelling/swollen glands
CVS: denies chest pain, palpitations, ankle swelling, PND, Orthopnea
Pulmonary: mild SOB denies cough
GI: denies N/V/D, constipation, abdominal pain, changes in Bowel Movement, bloating, anorexia, blood in stools, hemorrhoids
GU: Denies incontinence, dysuria, nocturia, urgency, flank pain, hematuria, urethral discharge
MSK: denies joint pain
Neurologic: Denies memory issues, HA, dizziness, slurring speech, paresthesia, paresis, tremors
Psychiatric: Denies depression, anhedonia, nightmares, suicidal or homicidal ideation.
Endocrine: Denies cold/heat intolerance, polyphagia, polydipsia
Heme: fatigue after long day of work. Denies fever, jaundice, generalized weakness, easy bruising or bleeding
Initial Differential Diagnosis:
- Benign thyroid nodule
- Thyroid cancer
- Subacute thyroiditis
- Goiter
- Hypothyroidism
- Advance reflex
- Benign Lesion
PE:
VS:
BP 120/ 70 mm Hg seated, right arm
T 98.2, oral
HR 86bpm regular
RR 16 unlabored
SpO2 100% on RA
Ht 67”, Wt 135 lbs, BMI 21.1 – hasn’t changed in 6 months
Gen: Well-developed female. Alert and oriented x 3, Not in any apparent Distress, Compliant to exam. Dressed and groomed appropriately.
Skin: Warm and dry, good turgor
Head: Normocephalic and atraumatic
Eyes: clear sclera and conjunctivae, PERRLA, EOMs full without nystagmus
Ears: hearing intact to whisper test, clear canals. Slight cerumen present in both canals, but TMs visualized and without lesions.
Mouth/Throat: Oral mucosa moist and pink. Mild periodontal disease noted. Tonsils are normal in size, free of exudates. Oropharynx normal. Tongue midline. Uvula rises symmetrically, tongue protrudes in midline
Neck: supple, no JVD. Carotids 2+ without bruits but a 2-cm firm, nontender nodule
in the right lobe of the thyroid gland was palpable, no movement with swallowing
lymphadenopathy was not evident
Heart: RRR, Normal S1 and S2, no Murmur/Rubs/Galaps noted
Lung: Clear to auscultation, no accessory muscle use
Abd: soft, non-tender. No masses, lesions, or pulsations noted. No organomegaly. Liver edge firm. No guarding or rebound tenderness
GU: No inguinal adenopathy, no suprapubic tenderness. Genital and rectal exam deferred
MSK: Grossly normal with good ROM all 4 extremities. No joint swelling or deformity
CN: a V1-V3 intact, no facial asymmetry, equal elevation of palate
Motor: normal bulk and tone. Strength symmetric. No tremors. No pronator drift
Sensory: to pinprick intact all 4 distal extremities
DTR’s: 2+ throughout. No clonus. Toes down-going, Gait normal
Extremities: No edema, clubbing, cyanosis
Labs: CBC, CMP, TSH, T4, Thyroglobulin Level, calcitonin
CBC and CBP with in normal limit
TSH- 1.8 [normal]
T4- 6.2 [normal]
Free T3- 300 pg/ml
Free T4- 1.0 ng/dL
ALL the lab tests were within normal limits.
Imaging:
Ultrasound- to confirm the presence of mass
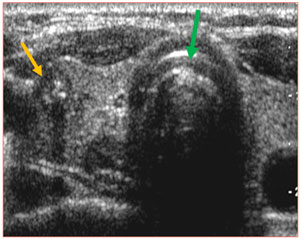
The green arrow shows the trachea and the yellow arrow shows a nodule in the right thyroid gland.
Impression of the US: The ultrasonography (US) showed a solid, irregular margin nodule, 2.5 cm in size, in the right lobe of the thyroid. accompanying microcalcifications and hypoechogenicity
Ultrasound-guided Fine-needle aspiration biopsy: suspicion for malignant papillary carcinoma
A single fine-needle aspiration biopsy of the right lobe nodule revealed microscopic appearance of a papillary carcinoma showing well-formed papillae and cells with ground glass nuclei.
DDX: Papillary Thyroid Cancer
Management
Treatment depends on the type of cancer and prognosis depends on staging, with a 99% 5-year survival with locally confined, less than 1 cm papillary carcinoma.
- Always involves complete or partial removal of the thyroidwith chemotherapy and external beam radiation reserved for anaplastic thyroid cancer
Sources:
- https://www.cancer.net/cancer-types/thyroid-cancer/diagnosis
- https://www.endocrineweb.com/conditions/thyroid-cancer/thyroid-cancer-symptoms
- https://www.endocrineweb.com/conditions/thyroid-cancer/papillary-cancer
- randon, David C., et al.. “Introduction to Nuclear Medicine.” Introduction to Diagnostic Radiology Eds. Khaled M. Elsayes, and Sandra A. A. Oldham. New York, NY: McGraw-Hill, 2014, http://accessmedicine.mhmedical.com.york.ezproxy.cuny.edu/content.aspx?bookid=1562§ionid=95875470.
- Thyroid Cancer. In: Papadakis MA, McPhee SJ, Bernstein J. eds. Quick Medical Diagnosis & Treatment 2020 New York, NY: McGraw-Hill; . http://accessmedicine.mhmedical.com.york.ezproxy.cuny.edu/content.aspx?bookid=2750§ionid=231382022. Accessed May 06, 2020.
- Fitzgerald, Paul A.. “Thyroid Cancer.” Current Medical Diagnosis and Treatment 2020 Eds. Maxine A. Papadakis, et al. New York, NY: McGraw-Hill, , http://accessmedicine.mhmedical.com.york.ezproxy.cuny.edu/content.aspx?bookid=2683§ionid=225134229.
- https://smartypance.com/lessons/endocrinology/thyroid-carcinoma/
- https://labtestsonline.org/conditions/thyroid-cancer
- https://www-uptodate-com.york.ezproxy.cuny.edu/contents/papillary-thyroid-cancer-clinical-features-and-prognosis?search=Thyroid%20Cancer&source=search_result&selectedTitle=2~150&usage_type=default&display_rank=2#H8
- https://jmedicalcasereports.biomedcentral.com/articles/10.1186/1752-1947-1-133

This entry is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International license.